Wed 21 Apr 2021
Covid-19 has been challenging for everyone, however adapting to this ‘new normal’ has been particularly difficult for Schools, Nurseries and Childcare providers. It is extremely difficult for very young children to understand the concept of social distancing.
Safely returning children to educational and childcare settings has been a vital part of easing restrictions and restarting the economy. However, it remains vital that everyone continues to take appropriate precautions to avoid a resurgence of the virus.
This article seeks to provide clear direction to staff working in childcare settings on infection control, first aid and resuscitation in a childcare and educational setting.
The Government has published detailed guidance on preparing for the wider opening of early years and childcare settings, Actions for schools during the coronavirus (COVID-19) outbreak and guidance for special schools, specialist colleges, local authorities and any other settings. This guidance will be regularly updated.
Effective infection control measures
It is vital that all staff and parents work together to help prevent the resurgence of the virus.
In all education, childcare and social care settings, preventing the spread of coronavirus (COVID-19) involves preventing direct transmission (by avoiding close contact with anyone potentially infected who is sneezing and coughing) and indirect transmission (via touching contaminated surfaces).
It is critical that everyone takes the same precautions and approach in attempting to reduce the spread of the virus:
minimise contact with anyone who is unwell by ensuring that those who have coronavirus (COVID-19) symptoms, or who have someone in their household who does, do not attend the childcare settings–all staff should be undertaking regular lateral flow testing and must declare any changes to their Coronavirus status on a daily basis.
clean hands more often than usual - wash hands thoroughly for 20 seconds with running water and soap and dry them thoroughly or use alcohol hand rub or sanitiser ensuring that all parts of the hands are covered. Childcare settings will need to provide hand sanitiser and additional hand washing stations to facilitate this. It is vital that everyone continually reinforces the importance of hand and respiratory hygiene and facilitate times for handwashing throughout the day.
continue to ensure good respiratory hygiene by promoting the ‘catch it, bin it, kill it’ approach –all childcare settings should have a lidded bin and this must be emptied regularly throughout the day.
cleaning frequently touched surfaces often using standard products, such as detergents and bleach – It will be necessary for most childcare settings to increase their cleaning regime and provide staff with suitable wipes and cleaning materials to maintain the necessary level of infection control. COVID-19: cleaning of non-healthcare settings guidance
High traffic areas and regularly touched items such as light switches, computer screens and mice, doorknobs, lift buttons, bannisters, taps, loo flushes etc should all be cleaned on a regular basis.
Children should have their own pencils, books, toys etc and avoid sharing any equipment wherever possible. If it is essential that if equipment is shared and cannot easily be cleaned, that it should be appropriately quarantined.
minimising contact and mixing by altering, as much as possible, the environment (such as classroom layout) and timetables (such as staggered break times)
Classrooms should be well ventilated, and outdoor space should be used whenever possible.
Personal protective equipment (PPE) including face coverings and face masks
The Government state that the majority of staff in education settings will not require PPE beyond what they would normally need for their work, even if they are not always able to maintain a distance of 2 metres from others. PPE is only needed in a very small number of cases including:
children whose care routinely already involves the use of PPE due to their intimate care needs should continue to receive their care in the same way.
if a child becomes unwell with symptoms of coronavirus (COVID-19) while in their setting and needs direct personal care until they can return home. A fluid-resistant surgical face mask should be worn by the supervising adult if a distance of 2 metres cannot be maintained. If contact with the child is necessary, then disposable gloves, a disposable apron and a fluid-resistant surgical face mask should be worn by the supervising adult. If a risk assessment determines that there is a risk of splashing to the eyes, for example from coughing, spitting, or vomiting, then eye protection should also be worn – childcare settings will need to invest in this PPE to ensure it is available if needed.
If the potentially infected person coughs or sneezes into a tissue, this should be double bagged and ideally disposed of in a sanitary bin for incineration.
Impact on employers and childcare businesses
The Department for Business (BEIS) and Public Health England have issued guidance for employers which is useful for Childcare businesses with employees.
For Childminders and smaller childcare businesses, it is vital to ensure your Terms and Conditions clearly state what has been agreed when children are ill, staff are ill, or the childcare provision is forced to close. This will determine whether or not parents are still responsible for fees in these circumstances.
What happens if someone becomes unwell with Covid symptoms in an educational or childcare setting?
If anyone in an education or childcare setting becomes unwell with Covid-19 symptoms, such as; a new, continuous cough or a high temperature, or change in normal sense of taste of smell (anosmia), they must be sent home and advised to follow the COVID-19: guidance for households with possible coronavirus (COVID-19) infection guidance.
If a child is awaiting collection, they should ideally be isolated from others in a well-ventilated room. If it is not possible to isolate them, they should be re-located to an area at least 2 metres away from other people.
If they need to go to the bathroom while awaiting collection, they should use a separate bathroom if possible. The bathroom should be cleaned and disinfected using standard cleaning products before being used by anyone else.
PPE should be worn by staff caring for the child while they await collection.
In an emergency, call 999 if they are seriously ill or injured or their life is at risk – state that you suspect Covid-19.
If a member of staff has helped someone with symptoms, they do not need to go home unless they develop symptoms themselves. They should wash their hands thoroughly for 20 seconds after contact with someone who is unwell. It is vital that any contaminated areas are thoroughly cleaned once the patient has left,
What if a child requires first aid?
If a child in your care requires first aid (and they do not have Covid symptoms), you should administer appropriate first aid to them as you would have done pre-Covid.
What if a child is unconscious and not breathing and needs CPR?
Resuscitation Council UK and the following Government guidance https://www.gov.uk/government/publications/novel-coronavirus-2019-ncov-interim-guidance-for-first-responders/interim-guidance-for-first-responders-and-others-in-close-contact-with-symptomatic-people-with-potential-2019-ncov
The following temporary CPR advice specifically for Covid-19:
During the Covid-19 pandemic:
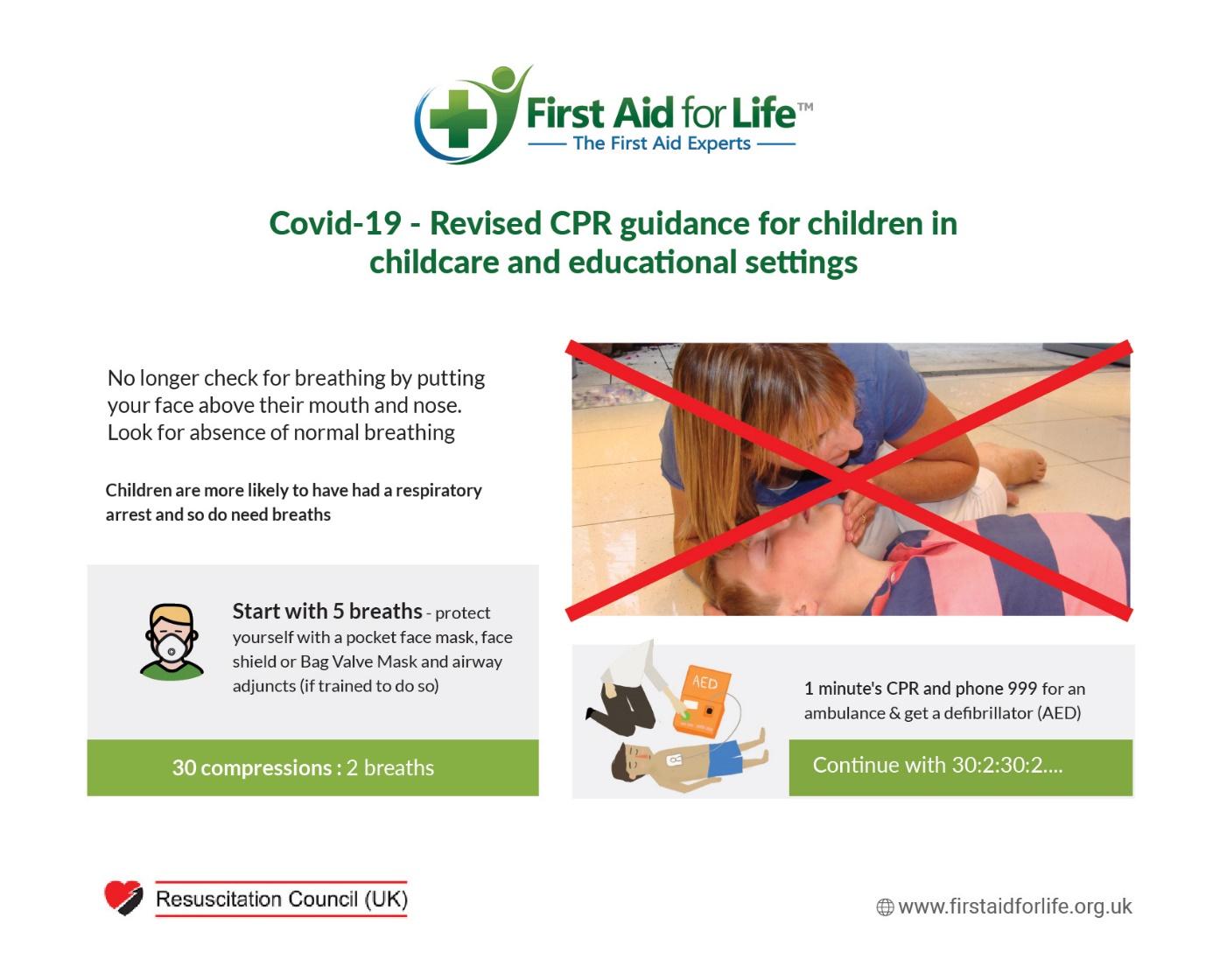
During Covid-19, it is no longer advised to look listen and feel with your head above their mouth and nose, in order to establish if they are breathing normally. Instead, you should recognise cardiac arrest by looking for the absence of signs of life and absence of normal breathing. If you are in any doubt whether or not they are breathing normally, start chest compressions until help arrives.
Call 999 for an ambulance and advise the emergency service if COVID 19 is suspected.
If there is a perceived risk of infection, place a cloth/towel over the victim’s mouth and nose and start compression only CPR and early defibrillation until the ambulance arrives. Place hands on the centre of the chest and push hard and fast.
Early use of a defibrillator (AED) significantly increases the person’s chances of survival and does not increase risk of infection.
Wear personal protective equipment (PPE), such as gloves and face mask, if possible.
After performing compression-only CPR, all rescuers should wash their hands thoroughly with soap and water or use alcohol-based hand gel. They should also seek advice from the NHS 111 coronavirus advice service or medical adviser.
Covid-19 advice for a child who is unconscious and not breathing:
The Government gives the following advice: https://www.gov.uk/government/publications/novel-coronavirus-2019-ncov-interim-guidance-for-first-responders/interim-guidance-for-first-responders-and-others-in-close-contact-with-symptomatic-people-with-potential-2019-ncov:
Cardiac arrest in children is more likely to be caused by a respiratory problem (asphyxial arrest), therefore chest compressions alone are unlikely to be effective.
If a decision is made to perform mouth-to-mouth ventilation in asphyxial arrest, use a resuscitation face shield where available.
Should you have given mouth-to-mouth ventilation there are no additional actions to be taken other than to monitor yourself for symptoms of possible COVID-19 over the following 14 days. Should you develop such symptoms you should follow the advice on what to do on the NHS website.
Resuscitation Council UK give more detailed guidance:
“We are aware that paediatric cardiac arrest is unlikely to be caused by a cardiac problem and is more likely to be a respiratory one, making ventilations crucial to the child’s chances of survival. However, for those not trained in paediatric resuscitation, the most important thing is to act quickly to ensure the child gets the treatment they need in the critical situation.
For out-of-hospital cardiac arrest, the importance of calling an ambulance and taking immediate action cannot be stressed highly enough. If a child is not breathing normally and no actions are taken, their heart will stop and full cardiac arrest will occur. Therefore, if there is any doubt about what to do, this statement should be used.
It is likely that the child/infant having an out-of-hospital cardiac arrest will be known to you. We accept that doing rescue breaths will increase the risk of transmitting the COVID-19 virus, either to the rescuer or the child/infant. However, this risk is small compared to the risk of taking no action as this will result in certain cardiac arrest and the death of the child”.
Further to the above advice, the following statement was issued by Resus UK, in direct response to a letter from the Group Health and Safety Manager at the Harris Federation requesting clarification on this topic:
Resuscitation Council UK Paediatric Guidance was written with the general public in mind as we know that many sudden cardiac arrests occur in the home hence: It is possible that the child/infant having an out-of-hospital cardiac arrest maybe known to you.
However, we recognise that in the school situation this may not always be the case. In this instance, the actions taken by the rescuer would be guided by dynamic/rapid risk assessment, considering such factors as the history of the child’s collapse and any known medical history, the presence or otherwise of COVID–19 signs/symptoms and the medical history of the rescuer.
We accept that doing rescue breaths will increase the risk of transmitting the COVID-19 virus, either to the rescuer or the child/infant (hence the need for a rapid dynamic risk assessment at the point of collapse). If the decision is to give rescue breaths, this may be mitigated by the use of airway adjuncts such as face shield, pocket mask or bag-valve-mask device if training has been received in the use of such devices. The choice of airway adjunct is dependent on the local environment, the level of training available to staff, and local supply chains.
About us
First Aid for Life provide award-winning, covid-secure first aid training tailored to your needs. They specialise in Paediatric First Aid training.
Please join us for one of our fully regulated Practical, Blended or Online First Aid courses. Please visit https://firstaidforlife.org.uk or call 0208 675 4036 for more information.
First Aid for Life is a multi-award-winning, fully regulated first aid training provider. Our trainers are highly experienced medical, health and emergency services professionals who will tailor the training to your needs. Courses for groups or individuals at our venue or yours.
First Aid for life provides this information for guidance and it is not in any way a substitute for medical advice. First Aid for Life is not responsible or liable for any diagnosis made, or actions taken on this information.